
I want to be honest with all of you, as you have all been with me through this journey so far. The last couple of weeks have been really overwhelming, and it has been really difficult to find topics that excite me in the medical world. Everything feels so stressful and exhausting. With information access being at an all-time high, it can feel really difficult to keep up with what’s relevant, important, and not false. I also feel like everything in the medical world is so negative right now, and information feels more like fear-mongering than helpful information. I don’t want to be another voice like that, sharing information that is scary rather than helpful, so I’m going to continue to be honest with you all and only share information I personally believe is worth sharing. For that reason, I hope you enjoy today’s blog entry! We’re going to learn more about a medical condition that isn’t always spoken about, but is definitely worth talking about. However, it’s not going to be the same kind of “disease profile” post I usually write.
Recently, I’ve been thinking a lot about strokes and how they come about, what factors can increase your risk of having a stroke, and so on. This led to a very deep dive into different medications that can contribute to the development of stroke. Now, I would like to preface this by saying I am in no way telling you these medications “cause” stroke (I need to make that very clear); I have just explored different research articles and studies which have evidence for links between these medications and stroke. Some of these medications are more readily accepted as increasing the risk of stroke, while others are suspected, but there is no evidence to confirm this.
A quick overview of the definition of stroke and its main causes
I will not be able to fully describe what a stroke is in this little section because stroke, in itself, is a very broad speciality in medicine. Understanding stroke in totality is just something that may never happen, but there are some very dedicated doctors who have devoted their lives to supporting patients, specifically those who have had a stroke, and they are much more knowledgeable about the topic than I am. Instead, I can provide you with a brief summary of what stroke is, to help with understanding how the following medications can be linked with the disease.
Stroke is defined as “a syndrome of acute, focal neurological deficit attributed to vascular injury of the central nervous system” (1,2). Put more simply, a stroke is a collection of specific symptoms that are caused when a part of the brain or spinal cord becomes damaged. This damage occurs when a part of the brain or spinal cord is not receiving enough blood, either because the blood vessel is blocked or because blood is leaking out of the blood vessel somewhere. The symptoms of stroke last more than 24 hours, or until the person passes away, unfortunately.
There are two main types of stroke (and some other, more niche types, which may be discussed in another article). These are:
- Ischaemic stroke — this is a stroke caused by a blocked blood vessel. This stops the blood from reaching the parts of the brain or spinal cord it needs to, and these parts begin to die. This accounts for almost 85% of all strokes.
- Haemorrhagic stroke — this is a stroke caused by a blood vessel bursting and leaking blood. Again, this stops an adequate amount of blood from reaching specific parts of the brain and spinal cord, leading to these parts dying. This accounts for almost 15% of strokes worldwide.
It is important, I feel, to mention Transient Ischaemic Attacks (TIAs), which are popularly known as “mini-strokes”. These are similar to stroke, except that the blockage in the brain or spinal cord, which causes the symptoms seen in this condition, becomes unblocked, and so the symptoms last less than 24 hours.
The main root causes for most strokes are high blood pressure (hypertension), blood clots forming more easily, or blood vessel narrowing. Figure 1 shows how each one can lead to blood vessel blockage or leaking. High blood pressure can cause damage to blood vessels in different ways, as mentioned in a past article (https://staymeducated.com/pressure-you-just-cant-ignore-it/). Blood clots can clearly lead to blockages in blood vessels because, if they get big enough, they will obstruct the flow, as seen in the diagram. Blood vessel constriction or narrowing can cause blockages because smaller blood clots or other substances in the blood can get stuck in the smaller, narrower sections, causing a blockage. Narrow or constricted blood vessels can also lead to leakage because the blood vessels can bulge behind the narrow sections and eventually burst from the increased blood pressure in these bulging areas.
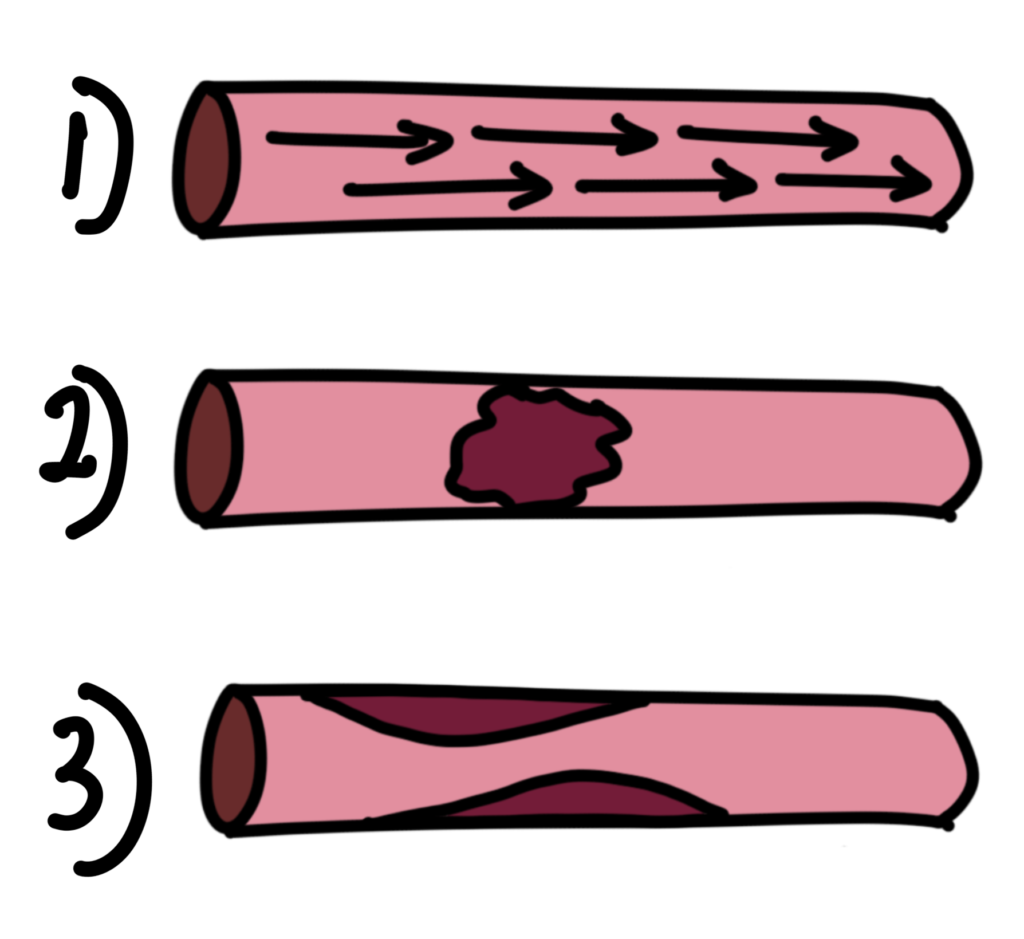
Figure 1 — Three different diagrams of the main causes of blood vessel blockage or leakage. 1) demonstrates high blood pressure through a blood vessel. 2) demonstrates a blood clot inside a blood vessel, and 3) demonstrates narrowing within a blood vessel. Created by Dr Mojibola Orefuja.
This is a VERY brief overview of some of the introductory points in stroke medicine, but hopefully this helps make more sense of the rest of the article.
When thinking about medications that can contribute to the development of stroke, the theory is that they affect one of the above-mentioned main causes. Theories suggest that these medications may increase blood pressure, increase the chances of forming blood clots, or cause blood vessel narrowing and constriction, all of which could lead to a stroke if there are other predispositions and risk factors present. A study in 2021 (3) set out to establish whether over 80 medications had substantial effects on the development of ischaemic stroke (IS). They grouped the medications into 11 chemical groups, including “drugs used for the respiratory system”, “anti-parasitic products, insecticides and repellents”, “systemic hormonal preparations”, and more. Their study revealed at least 7 medications with high levels of evidence supporting an association with the development of stroke, while 36 medications did not have enough evidence to suggest a link to stroke. This study also revealed that there is a relative risk associated with all medications, dependent on the age, gender, and other medical conditions a person has when taking these “risky” medications. I’m going to go through the main medications spoken about in this study.
Oral Contraceptives and Other Hormonal Medications
It is a long-known fact that oral contraceptives can contribute to the development of stroke because they can increase blood clot formation in the body. By increasing blood clots, this raises the risk of blocked blood vessels, which leads to stroke. Study 4 found that when patients were on oral contraceptives at high doses, this increased the risk of stroke in women. Results also showed that when women stopped using oral contraceptives, their risk of stroke was reduced (4). Other studies have further supported this theory of oral contraceptives increasing stroke risk through an increased risk of blood clots, as seen in source 5. However, source 5 also shows that the use of oral contraceptives can be linked to an increased risk of other cardiovascular risk factors, like high cholesterol. Studies do, however, continue to stress that the associated risk of stroke from oral contraceptives is strongly linked to age and other medical conditions and risk factors present when taking contraceptives (6), so it’s important to make sure that this is considered before starting or stopping them.
Antipsychotics
Antipsychotic medications sound a bit more dramatic than they actually are. Yes, they do help with psychosis, but they also help with lots of other mental health and neurological conditions like depression, dementia, bipolar disorder, and some personality disorders. A meta-analysis carried out in source 7 shows that there is a significant link between the use of antipsychotics and an increased likelihood of having a stroke. The study did show, however, that there was a change in relative risk when assessing the risk in patients with dementia. This is because studies weren’t able to properly link stroke development to the use of antipsychotics rather than to the presence of dementia. Source 8 also found that there is a slightly higher risk of developing stroke when using atypical antipsychotics than with typical antipsychotic medications (8,9). This is further supported by the study carried out in source 9. This study found that the risk of stroke increased by 1.45 times when a person was using a second-generation (atypical) antipsychotic medication. This risk also varied depending on the age of the patient. Antipsychotic medications have been associated with increased stroke risk because some antipsychotics have the side effect of increasing cholesterol and lipid levels in the blood, which can lead to blocked blood vessels.
Erythropoietin
Erythropoietin is a protein made in the kidney which is released into the blood to promote the development of blood cells when parts of the body need oxygen. Erythropoietin is produced naturally in the body when stimulated, but there is also a synthetic version which can be used for people with blood disorders and other types of diseases. There are studies which support the use of erythropoietin in stroke patients, while some studies also suggest that erythropoietin can actually contribute to stroke risk (10). As erythropoietin is used to increase blood cells in the body, it is proposed that its use in post-stroke patients will promote good blood supply to the damaged parts of the brain or spinal cord (10). However, before a stroke occurs, it is thought that because erythropoietin increases blood cell formation, it increases the risk of blood clots, which are associated with stroke (12). There is, unfortunately, no significant evidence or studies carried out to explore the actual effects of erythropoietin on the development of stroke.
Now, I know this topic is a bit random, but I hope you learned something new, like I did when I took this deep dive. Which medication, or group of medications, surprised you the most from the article?
References:
- Murphy SJX, Werring DJ. Stroke: causes and clinical features. Medicine (Abingdon). 2020 Sep;48(9):561–566. doi:10.1016/j.mpmed.2020.06.002
- Wang D, Dong Y, Wang Y. Ischemic stroke [Internet]. BMJ Best Practice; 2025 [updated 2025 Oct 14; cited 2026 Apr 17]. Available from: https://bestpractice.bmj.com/topics/en-gb/1078
- Marto JP, Strambo D, Livio F, Michel P. Drugs associated with ischemic stroke: a review for clinicians. Stroke. 2021 Oct;52(10):e646–e659. doi:10.1161/STROKEAHA.120.033272
- Xie Z, Li Z, Liu F, Luo H, Han H, Qin Y, et al. Oral contraceptive use and increased risk of stroke: a dose–response meta-analysis of observational studies. Front Neurol. 2019;10:993. doi:10.3389/fneur.2019.00993
- Strambo D, Sirimarco G, Nannoni S, Dunet V, Michel P. Ischemic stroke on hormonal contraceptives: characteristics, mechanisms and outcome. Eur Stroke J. 2021 Jun;6(2):156–165. doi:10.1177/23969873211019586
- WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Haemorrhagic stroke, overall stroke risk, and combined oral contraceptives: results of an international, multicentre, case-control study. Lancet. 1996 Aug;348(9026):505–510. doi:10.1016/S0140-6736(95)12394-6
- Zivkovic S, Koh CH, Kaza N, Jackson CA. Antipsychotic drug use and risk of stroke and myocardial infarction: a systematic review and meta-analysis. BMC Psychiatry. 2019 Jun 20;19(1):189. doi:10.1186/s12888-019-2177-5
- Douglas IJ, Smeeth L. Exposure to antipsychotics and risk of stroke: self controlled case series study. BMJ. 2008 Aug 28;337:a1227. doi:10.1136/bmj.a1227
- Liao YT, Yang SY, Liao SC, Kuo CJ. Antipsychotic medications and stroke in schizophrenia: a case-crossover study. PLoS One. 2017 Jun 14;12(6):e0179424. doi:10.1371/journal.pone.0179424
- Ma Y, Zhou Z, Yang GY, Ding J, Wang X. The effect of erythropoietin and its derivatives on ischemic stroke therapy: a comprehensive review. Front Pharmacol. 2022 Feb 17;13:743926. doi:10.3389/fphar.2022.743926
- Souvenir R, Doycheva D, Zhang JH, Tang J. Erythropoietin in stroke therapy: friend or foe. Curr Med Chem. 2015;22(10):1205–1213. doi:10.2174/0929867322666150114152134